
| Home Page | Overview | Site Map | Index | Appendix | Illustration | About | Contact | Update | FAQ |
|
|
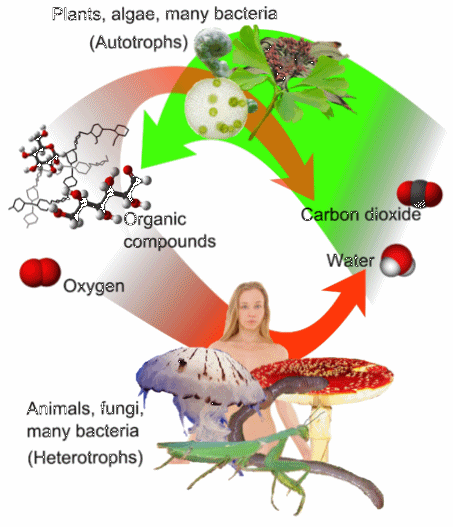
There are two types of living organisms in this world. The autotrophs (self-nourishment) live on inorganic materials, while the heterotrophs (different-nourishment) must make use of resource that comes from other organisms in the form of fats, carbohydrates and proteins (Figure 01). Thus, there is always an arm race going on for the latter type - it's a race between attack and defence (Figure 02). Such acts are all too obvious in the macroscopic setting, actually the same kind of struggle is on going all the time in the microscopic environment. The lower frame of Figure 02 shows a swarm of viruses (in blue) attacking an E. coli bacterium with the contractile sheath, which acts like a syringe to squirt the genetic material (DNA) into the host cell. |
Figure 01 Heterotrophs |
Figure 02 Attack and Defence [view large image] |
It responds by secreting enzyme to cleave or disable the foreign DNA or commits suicide to protect the rest of the population if worse comes to worst. |
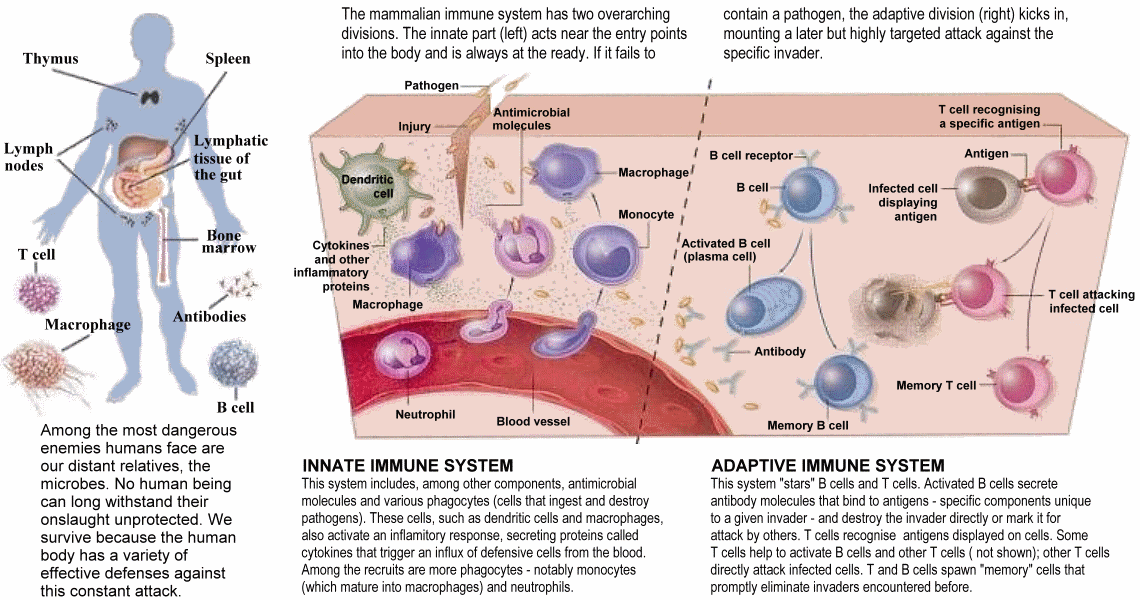 |
The subject on immune system in the followings is about the defence of an macroscopic being against the invasion of pathogenic microbes including bacteria, viruses, parasitic worms and fungi. Micro-organisms outnumber the human cells of our bodies by ten to one. Some of them are friendly (up to a point), doing us neither good nor harm, many are important to the functioning of the body, but there are nasty varieties that can cause all kinds of illness. The defence has to be able to tell friends from foes and also doesn't kill itself. The main lines of defence are the innate and adaptive immune systems (Figure 03) when the first line of defence crumbles under the assault. |
Figure 03 Immune Systems [view large image] |
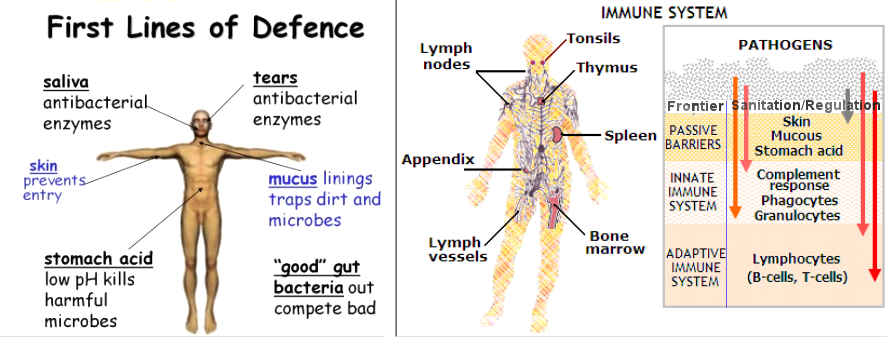 |
The first line of defence recruits helps with physical, chemical, and biological components. The methods are rather primitive, but all animals use them in one form or the others. A few of these are illustrated in Figure 04 (left frame). In addition to the three levels of defence as shown in the right frame, human culture/science has added a top layer by sanitating the environment, and by regulating the foods and drinks. |
Figure 04 First Line Defence |
The three components of the first line defence : |
 |
|
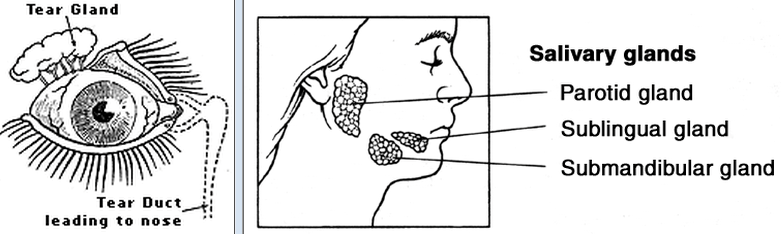
Figure 05 Physical Component |
|
 |
|
Figure 06 Antibacterial Emzyme [view large image] |
|
 |
|
Figure 07 Pore-forming Peptide [view large image] |
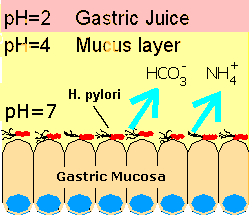 |
|
Figure 08 Gastric Acid |
|
 |
 |
anatomical sites on and in the human body and a short description of their functions. The bacteria in each site compile a micro-ecosystem (called microbiome) with the members link together and interact with the environment on or in the host. The microbiome behaves very similar to the macroscopic ecosystem, which exists in equilibrium even under small |
Figure 09a Good Bugs [view large image] |
Figure 09b Microbiome |
perturbation, except that it can respond quickly to change and different composition could perform the same funtion (to the host). |
 |
resistant. Common side effects include diarrhoea, hypersensitivity, nausea, rash, neurotoxicity, urticaria, and superinfection. Other antibiotics include Cephalosporins, Aminoglycosides, Tetracyclines, ... With advances in medicinal chemistry, most modern antibacterials are semisynthetic modifications of various natural compounds. These germ killing products, which are not produced by micro-organisms, such as proflavine, sulfonamide, ... are referred to as antibacterial drugs. |
Figure 09c Penicillin [view large image] |
It is found that antibiotic use (or mis-use) severely disrupts the microbiome (the micro-ecosystems on and in our body), causing extensive collateral damage. The indiscriminate killing of nonpathogenic members makes it easier for pathogens to invade otherwise stable, occupied environments. |
 |
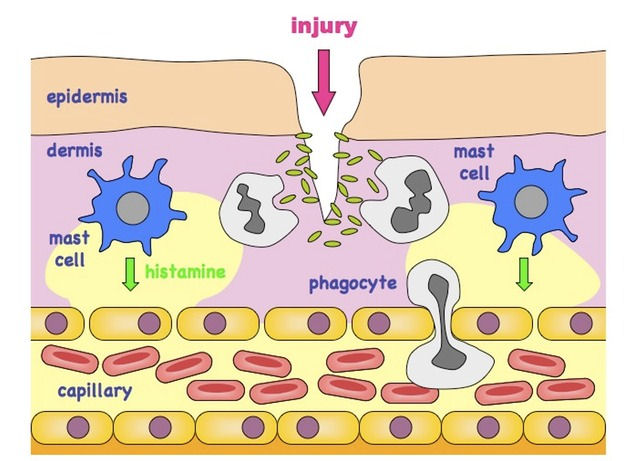 |
The white blood cells (leukocyte) are either amoeba-like single cells for devouring foreign substances or protista with granular chemicals on the surface for combating intruders (by releasing the chemicals). Figure 10 shows some of the different varieties. The upper frame in the image shows a macrophage in the process of devouring some E.coli bacteria, while the lower frame lists some of the various kinds of white blood cells. Essentially, there are two main types - phagocytes for the 2nd line of defence and lymphocytes for the 3rd line of defence. Both of them originate in the bone marrow. |
Figure 10 Phagocytes [view large image] |
Figure 11 2nd Line of Defence [view large image] |
 |
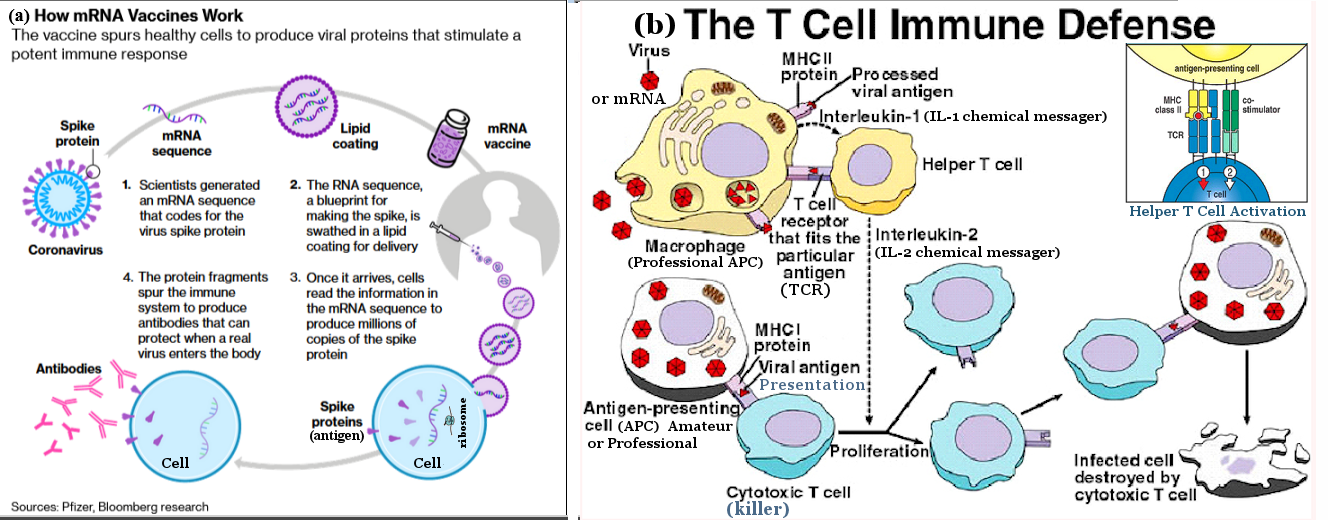
Since small unicellular organisms such as the viruses can alter their genes and appearance rapidly, no macroscopic animals can keep up with the pace correspondingly. Together with the innate immunity, the adaptive immune system has been evolved in vertebrates to deal with this problem. It is based on the "lock and key" mechanism that allows the generation of receptor that fit into the special feature on the pathogenic surface as illustrated in the left frame in Figure 13a. Fragments can also be manufactured by macrophage (and dendritic cell, ...) and presented to the B and T-helper cells (Figure 13a, right frame) for recognition. The helper (CD4+) T cells summon macrophages and neutrophils to the site of infection, while the cytotoxic (CD8+) T cells kill the pathogens directly. |
Figure 12 T and B Cells |
Vaccination is the administration of antigenic material (such as fragments of pathogenic protein, or a harmless or weakened strain - the vaccine) to stimulate the immune system for developing adaptive immunity with a pathogen. See lot more details in "Antibody". |
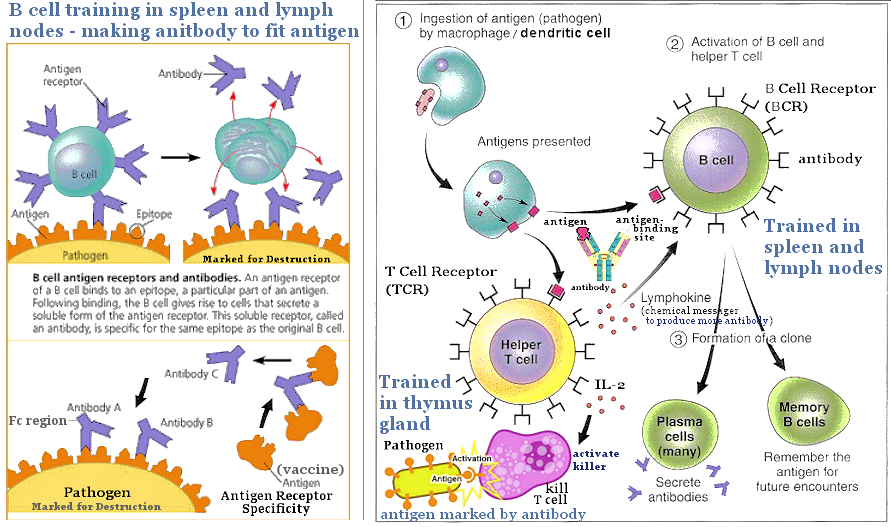 |
The differentiation continues after they have left the thymus. Those T cells would commit suicide if the antigen receptor do not fit any cell surface protein because they will be useless. Those with strong binding also kill themselves because the fragments are certainly to be normal human material, this is the way the immune system avoids acting against its own body. Thus, only those with weak binding survive, finish the education, and eventually enter into service carrying a memory of previous infection. Any pathogen with that particular fragment would be recognized quickly and disposed of. Figure 13a shows the training with pathogenic antigen. |
Figure 13a 3rd Line of Defence [view large image] |
BTW, "specificity" means an unique fit (see Figure 13a lower left), and lymphokine is protein mediator carrying various kinds of messages (Figure 13a,left); and it is now realized that T cells cannot recognize (and therefore cannot respond to) "free" or soluble antigens. |
 |
|
Figure 13b Antibody [view large image] |
See illustration and caption in Figure 13b,b. |
 |
entering the host cell by endocytosis. The DNA then replicates more of its kind and simultaneously making new coating proteins. These parts assemble to form more viruses, which exit from the host to infect more cells (Figure 14b). The RNA retrovirus (such as the coronavirus) does it somewhat differently because the genetic material is in the form of RNA. It has to undergo a reverse transcription to form cDNA (DNA copied off from the RNA), which is then integrated into the host DNA. It commandeers the host's replication mechanism to make more RNAs, which in turn make more coating proteins for the final assembly of new viruses. The followings provides further details on RNA virus replication in |
Figure 14 DNA Virus |
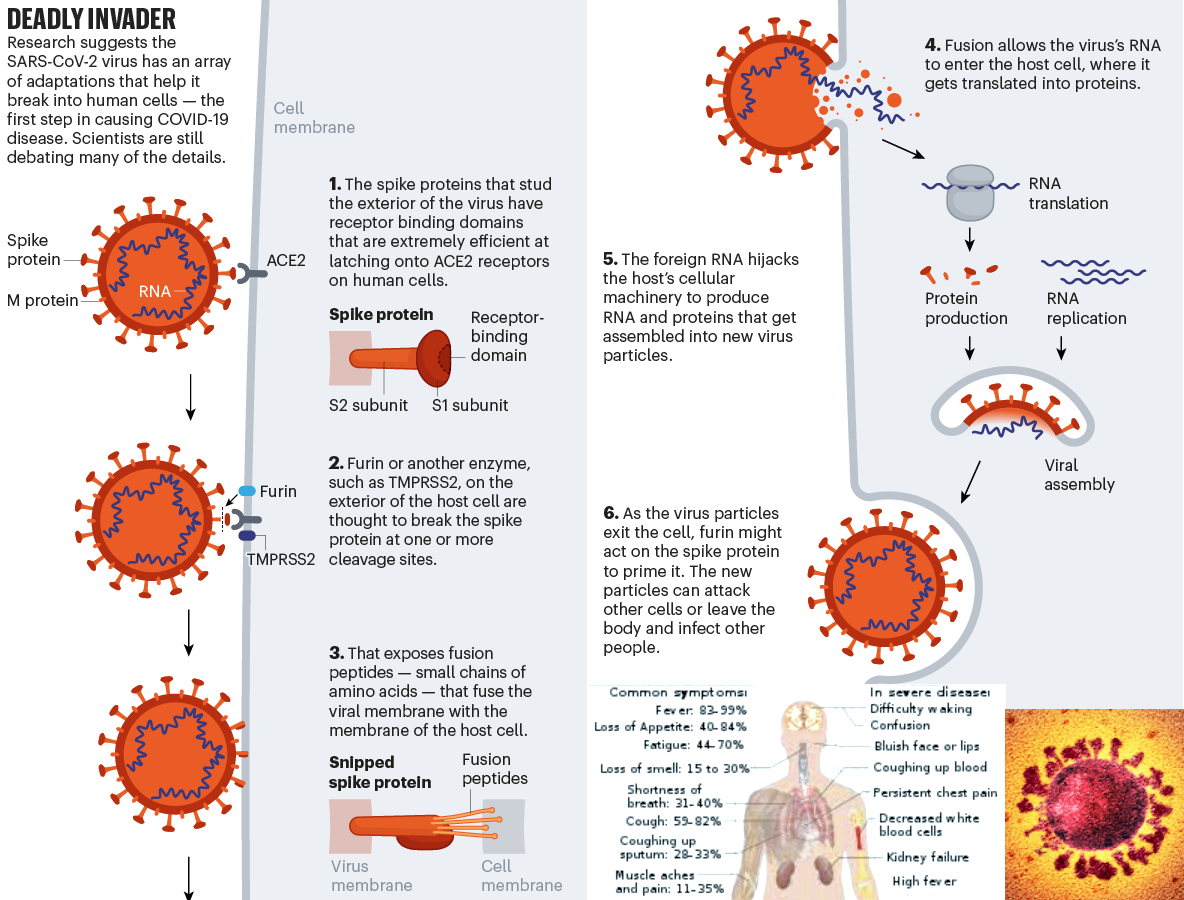
7 steps. There are numerous kinds of viruses, this summary only considers the single-stranded, positive-sense (its RNA is the same as mRNA) RNA virus (such as the Coronaviridae), which replicates solely in cytoplasm of the host cell (Figure 15). |
 |
|
Figure 15 RNA Virus |
 |
|
Figure 16a Covid-19, 2020 |
See original article : "Profile of a Killer" in Nature, 7 May 2020. |

 |
|
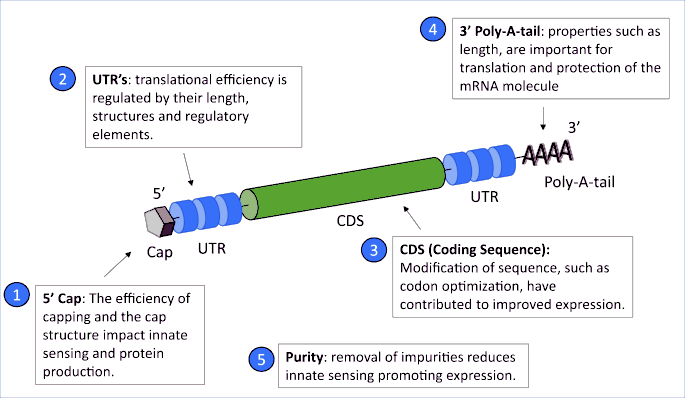
Figure 16c mRNA Structure |
The mRNA is unstable against decomposition, it must be stored at ultra-low temperatures of -80�C to -60�C up to the
end of its expiry date for a duration of 30 days. See more on the mRNA technology in "The promise of mRNA vaccines". |
 |
|
Figure 16d |
Vaccine Dilution [view large image] |
 |
markedly ~ 21 days after a first injection, suggesting limited survival and stimulation by the vaccine mRNA and its' encoded Spike protein beyond such time interval. However, the specific anti-viral immune response was strongly boosted with a 2nd injection of vaccine. This raises concerns that extending a second injection out to beyond ~ 21 days could compromise vaccine efficacy. The time interval for a mRNA booster may be very critical for getting the best sustained immune response. |
Figure 16e mRNA Vaccine and |
It is not known why the 2nd shot is so effective. Probably, it triggers the release of a lot more IL-2 chemical messagers by more helper T cells to proliferate and activate the killer T cells (see Figure 16e,b and update). |
 |
|
Figure 16f B Cell Activation |
destruction (e.g., by phagocyte, and see Figure 13a,left). It also serves as professional APC, secretes cytokines to activate the memory B cell and regulate the various components of the immune systrem (as shown in the update below, the process takes time to work). |
 |
|
Figure 16f2 Humoral Vaccination [image, video] |
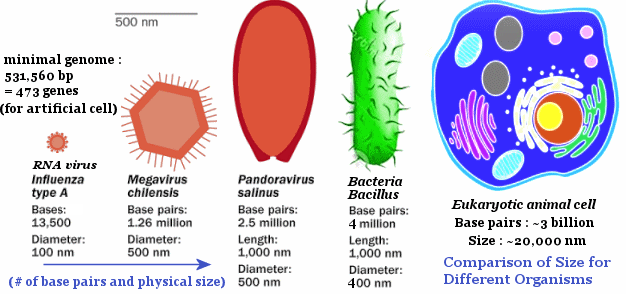 |
month. A mutation is an alteration in the sequence of nucleic acid in DNA or RNA caused by insertions, deletions, substitutions or rearrangements of bases. While most mutations are harmless (actually deleterious to the virus itself), a few can result in new proteins or altered cellular processing that turns it into more vicious variant. Naturally all organisms mutate in nature, the smaller genomic size makes the mutation in virus more noticeable (Figure 16g). Mutation is one of the elements in "Darwinian Evolution". |
Figure 16g Size of Organisms |
Figure 16k shows the genome of SARS2, and will be examined in details later, while Figure 16i illustrates some mutations in the spike protein. |
 |
|
Figure 16h Virus Infection with Proofreading [view large image] |
See the older version of Virus Infection in Figure 15. |
 |
See "Emerging SARS-CoV-2 Mutations and Variants". |
Figure 16i Mutations of Spike Protein |
Figure 16i shows the various kinds of spike protein variations in the B.1.1.7 (designated by some sort of convention, see "Lineage B.1.1.7") variant emerged at UK, and "Rare COVID reactions might hold key to variant-proof vaccines"; also a list of the amino acids. |
 |
logic, the SARS2 will follow a similar evolutionary trajectory of the 4 endemic (localized disease) coronaviruses that cause the �common cold�. It is possible that the virus has to change a little just to maintain itself in children (they typically have less severe disease than adults), or it may evolve to escape immunity by being able to better replicate in the nose and so turn into an upper respiratory infection, which makes the patient uncomfortable but not fatal. It is possible that SARS-CoV-2 vaccines will need to be updated, possibly every year like the flu vaccines. But even then, immunity from either past vaccination or infection will probably blunt serious disease. In case the SARS-CoV-2 vaccines block infection and transmission for life, the virus might become something akin to measles - two doses and a person is protected for life. |
Figure 16j Endemic SARS2 |
Figure 16j presents the result of a survey about the driving factor in endemic circulation. See original article : "The Coronavirus Will Become Endemic". |
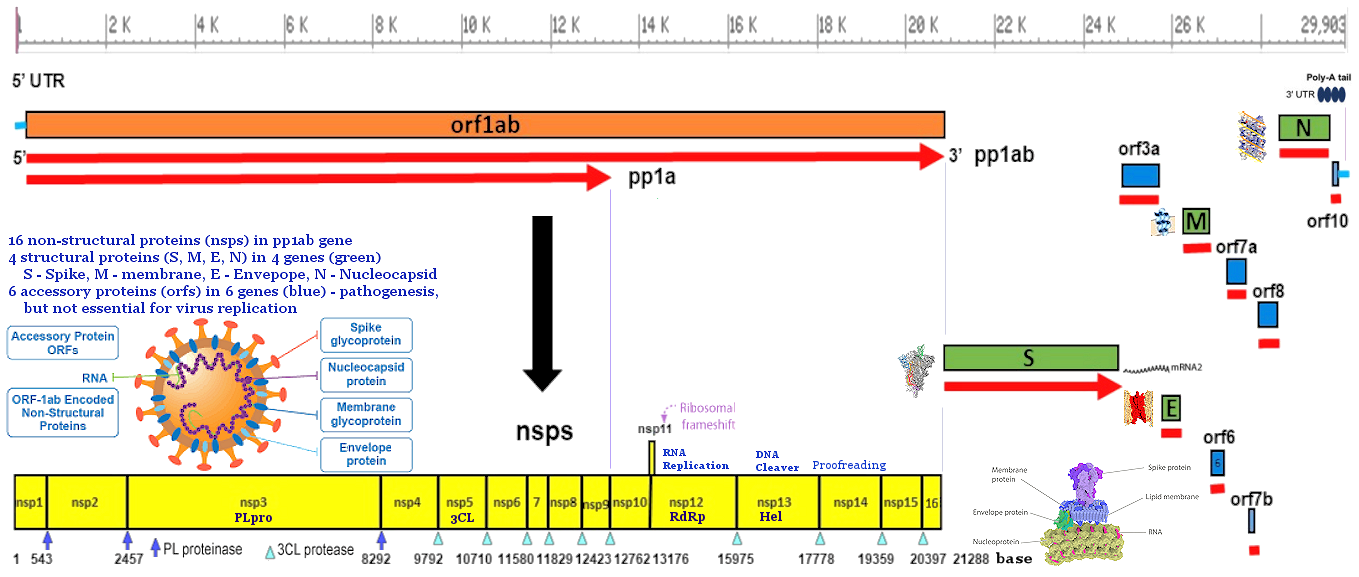 |
begins with a start codon (usually AUG or ATG) and ends at a stop codon (usually UAA, UAG or UGA). In eukaryotic genes with multiple exons, introns are removed and exons are then joined together after transcription (from DNA to RNA) to yield the final mRNA for protein translation. The orf1ab gene constitutes 2/3 of the SARS2 genome, encodes a total of 16 non-structural proteins (nsp's) within the pp1ab gene (pp = polyprotein) as shown in Figure 16k (yellow), and a table for nsp's. |
Figure 16k SARS2 Genome |

 |
reference, 38 recurrent non-synonymous mutations were identified. Among these mutations, 22 locate in the pp1ab nsp genes and 16 within the "more recent" additions of 4 structural genes. By taking into account the frequency of mutated alleles (= #-of- occurance/3067), the rate of mutation is > 0.28/month in the pp1ab and > 0.26/month in the structural genes for a total of > 0.54 mutations/month (see Figures 16l, and 16k, and compare to the 1 - 2 mutations/month quoted earlier). These numbers indicate that the mutations occur at random and the rate is much lower that the flu's 4 mutations/month (of genome size about 1/2 as much, see "Coronavirus seems to mutate much slower than seasonal flu"). |
Figure 16l SARS2 Variation |
And don't miss "Coevolution Scenario for the Virus and Cell". |
 |
On 20 August 2021, India�s drug regulator authorized the DNA vaccine for people aged 12 and older. The efficacy figure of 67% came from trials involving more than 28,000 participants, which saw 21 symptomatic cases of COVID-19 in the vaccinated group and 60 among people who received a placebo. The name of the product is ZyCoV-D (see Figure 16m). Here's a summary : |
Figure 16m ZyCoV-D [view large image] |
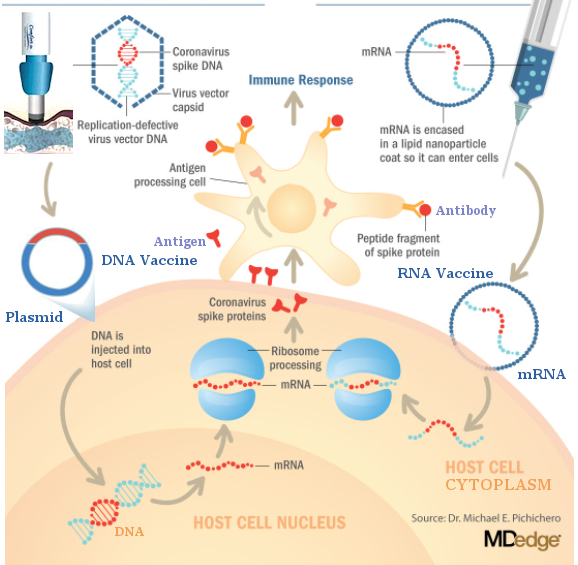 |
later than the other types and has only 67% efficacy (mainly against the Delta variant in the clinical trial). The problem is somehow solved by having the vaccine deposited under the skin. The area under the skin is rich in immune cells that gobble up foreign objects, such as vaccine particles, and process them. This helps the delivery far more efficiently than in the muscle. It is administered using a needle-free device pressed against the skin, which creates a fine, high-pressure stream of fluid that punctures the surface and is less painful than an injection. However, it requires a minimum of three doses to achieve its initial efficacy presenting certain logistical challenge, which may be neutralized by its more stable structure than mRNA vaccines. |
Figure 16n DNA Vaccine |
See original article : "India�s DNA COVID vaccine is a world first � more are coming". |
 |
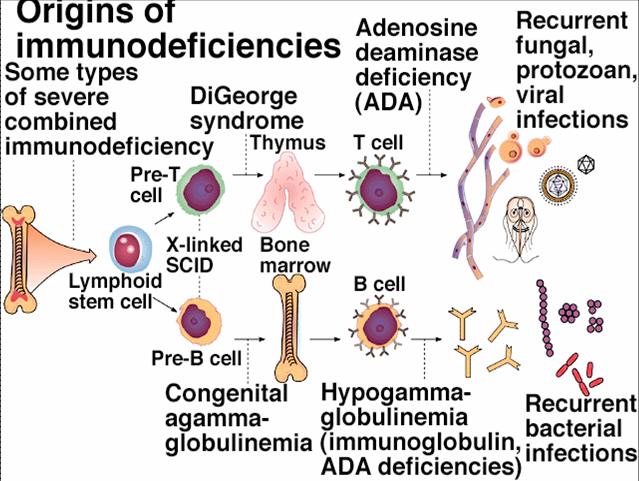 |
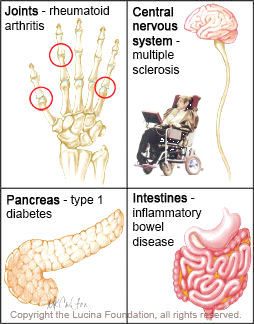
Immune system disorders are the abnormally over-activity or low activity of the immune system. In case of over-activity, the defence attacks and damages its own tissues. It is also known as auto-immune diseases (see Figure 15 for some examples). The treatment generally focuses on reducing immune system activity. Immune deficiency diseases decreases the body's ability to protect itself. Primary immuno-deficiency is cause by inherited genetic mutations (see Figure 16a for an example of mutation in the T and B cells), while secondary immuno-deficiency is the result of pathogenic intrusion. Table 01 lists some specific examples of the various disorders. |
Figure 17 Auto-immune Diseases |
Figure 18 Immunodeficiency, SCID [view large image] |
The "~ genetic" in the table signifies possible genetic mutation causing the failure. |
| Disease | Symptoms | Affected Body Parts | Failing Immune Components | Cure |
|---|---|---|---|---|
| Allergy | Runny nose, itchy eyes, and sneezing | Nose, lungs, eyes, and skin | Excessive activation of the mast cells and basophils by antibody (~ genetic) | Avoid the environmental or dietary allergens, take steroids to reduce immunity |
| Asthma | Wheezing, coughing, chest tightness, shortness of breath | Airways | Increase in eosinophils, macrophages, neutrophils, or T cells (~ genetic) | Avoid smoke, dust, fumes, take corticosteroids |
| Rheumatoid Arthritis | Inflammation, swelling and pain at the joints | Joints | Antibodies attach to the joints (~ genetic) | Antirheumatic drugs, exercise, surgery |
| Multiple Sclerosis (MS) | Pain, blindness, weakness, poor coordination, muscle spasms | Insulating covers of nerve cells in the brain and spinal cord | Destruction by the immune system (~ genetic) | No known cure |
| Type 1 Diabetes | Frequent urination, increased thirst, increased hunger, and weight loss | Pancreas | Antibodies attack and destroy insulin producing cells (genetic) | Immunosuppressive drugs, injections of insulin, pancreas transplantation |
| Inflammatory Bowel Disease (IBD) | Diarrhea, rectal bleeding, urgent bowel movements, abdominal pain, fever | Lining of the colon and small intestine | Immune system attacks elements of the digestive system (genetic) | Anti-inflammatory steroids, surgery |
| Severe Combined Immunodeficiency (SCID) | Vulnerable to infectious diseases | Defect in one of at least 9 possible genes | Absence of functional T cells leading to improper B cells activation (genetic) | Bone marrow transplantation. |
| Acquired Immune Deficiency Syndrome (AIDS) | Opportunistic infections and tumors | The whole body | Human immunodeficiency viruses (HIV) destroy T-helper (CD4) cells | No cure or vaccine, avoid unprotected sex and contaminated blood transfusions |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}